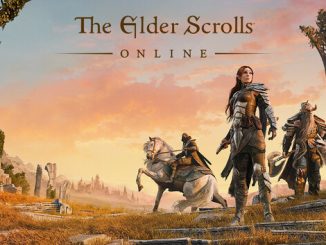
Fillin Station Diner: Tempat Makan Retro yang Harus Dikunjungi
Jika mencari-cari pengalaman makan kuliner yang spesial serta tak terlepas ingatan di tanah Indonesia, Restoran Fillin Station merupakan tempat untuk ideal untuk dikunjungi. Restoran ini […]